Rectum
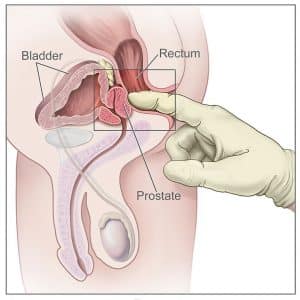
The anterior wall of the rectum has a number of close anatomical structures. These can therefore be palpated digitally via the rectum. Most significant are the prostate and seminal vesicles in males, and cervix in females. Bony structures, such as the sacrum and coccyx, may also be palpated in both sexes.




The rectum is the most distal segment of the large intestine, and has an important role as a temporary store of faeces.
It is continuous proximally with the sigmoid colon, and terminates into the anal canal.
1)sphincter tonus
2)діаметр отвору
3)взаємовідношення
4)стан кісткового апарату
The rectum begins at the level of the S3 (as a continuation of the sigmoid colon). It is macroscopically distinct from the colon, with an absence of taenia coli, haustra, and omental appendices.
The course of the rectum is marked by two major flexures:
- Sacral flexure – anteroposterior curve with concavity anteriorly (follows the curve of the sacrum and coccyx).
- Anorectal flexure – anteroposterior curve with convexity anteriorly. This flexure is formed by the tone of the puborectalis muscle, and contributes significantly to faecal continence.
There are additionally three lateral flexures (superior, intermediate and inferior), which are formed by transverse folds of the internal rectum wall.
The final segment of the rectum, the ampulla, relaxes to accumulate and temporarily store faeces until defecation occurs. It is continuous with the anal canal; which passes through the pelvic floor to end as the anus.
In the superior third of the rectum, the anterior surface and lateral sides are covered by peritoneum. The middle third only has an anterior peritoneal covering, and the lower 1/3 has no peritoneum associated with it.
In males, the reflection of peritoneum from the rectum to the posterior bladder wall forms the rectovesical pouch. In females, the peritoneum reflects to the posterior vagina and cervix, forming the rectouterine pouch (pouch of Douglas).


The rectum receives arterial supply through three main arteries:
- Superior rectal artery – terminal continuation of the inferior mesenteric artery.
- Middle rectal artery – branch of the internal iliac artery.
- Inferior rectal artery – branch of the internal pudendal artery.
Venous drainage is via the corresponding superior, middle and inferior rectal veins. The superior rectal vein empties into the portal venous system, whilst the middle and inferior rectal veins empty into the systemic venous system. Anastomoses between the portal and systemic veins are located in the wall of anal canal, making this a site of portocaval anastomosis.
Note: the rectum is also closely anatomically associated with the rectal venous plexus; however this structure is more functionally related to the anal canal.
- Sympathetic nervous supply to the rectum is from the lumbar splanchnic nerves and superior and inferior hypogastric plexuses.
- Parasympathetic supply is from S2-4 via the pelvic splanchnic nerves and inferior hypogastric plexuses. Visceral afferent (sensory) fibres follow the parasympathetic supply.
Lymphatic drainage of the rectum is via the pararectal lymph nodes, which drain into the inferior mesenteric nodes.
Additionally, the lymph from the lower aspect of the rectum drains directly into the internal iliac lymph nodes.
Palpation
- Lubricate your examination finger
- 2.Press your finger by the posterior anal edge
- Note any anal fissures that can be felt here
- 3.Gently insert your finger into the anal canal, following the natural curve of the sacrum
- Assess anal tone, also confirm by asking the patient to squeeze your finger
- 4.Carefully rotate your finger to feel all walls of the rectum
- This is best done by pronating at the wrist
- 5.In males, palpate the prostate on the anterior wall
- 6.Withdraw the finger and inspect contents for stool, blood, or mucus


Коментарі
Дописати коментар